∗Percentage of
concordant pairs

=
68.4%; percentage of
discordant pairs
=
10.6%; and percentage of
tied pairs
=
21.0%; Hosmer and Lemeshow goodness-of-fit test χ
2=
0.3733 (with 2 degrees of freedom);
p=
0.8297
>
0.05.
Article Outline
Abstract
Background
Epidermal growth factor receptor antagonists, such as gefitinib, erlotinib, and cetuximab, have been used in treating carcinomas. The efficacies have been proposed to correlate with skin reactions, but the most important predictive indicator is still unknown. Our aim was to investigate the types of skin toxicities and to analyze the major therapeutic predictive indicators in Taiwan.
Methods
A retrospective analysis was used to study 68 patients with advanced non-small-cell lung cancer receiving gefitinib.
Results
Acneiform eruption (41.2%), xerosis (38.2%), pruritus (26.5%), and paronychia (16.2%) composed most of the skin reactions. The univariate analysis revealed paronychia as the most substantial survival predictive indicator (
p=
0.0427). In the multivariate analysis, older patients with paronychia had better prognosis (
p=
0.0050). Women tended to develop paronychia (
p=
0.1098). Xerosis positively correlated with paronychia (
p=
0.0082).
Conclusion
Paronychia is the most indicative survival predictive factor among the skin manifestations, and it correlates with age, gender, and xerosis. Elucidation of the relationship between cutaneous reactions can provide information on the epidermal growth factor receptor signaling mechanism of skin.
Introduction
Gefitinib (AstraZeneca UK Limited, Cheshire, UK) is an oral anti-neoplastic agent classified as quinazoline. As a selective epidermal growth factor receptor (EGFR)–tyrosine kinase inhibitor (EGFR-TKI), it acts intracellularly to inhibit the EGFR signal transduction pathway. EGFRs are expressed in many solid tumors, such as those of lungs, breasts, stomach, colon, and pancreas.
1,
2 It may enhance carcinogenesis by promoting cell proliferation, motility, adhesion, invasive capacity, and inhibiting apoptosis.
1
It has been shown that gefitinib monotherapy has a significant antitumor effect in patients with advanced non-small-cell lung cancer (NSCLC).
3,
4,
5 Common cutaneous adverse reactions include acneiform eruption, xerosis, pruritus, and paronychia.
6,
7,
8 Several other studies have shown the possible relationship between the therapeutic efficacy and the severity of the cutaneous toxicities on treatment with EGFR antagonists, such as gefitinib, erlotinib, and cetuximab.
9,
10,
11,
12,
13,
14 We characterize the skin toxicities of gefitinib in Taiwan and investigate their roles in survival analysis.
Methods
Patients
From February 2003 to December 2004, 68 patients with NSCLC receiving gefitinib monotherapy more than 28 consecutive days in the National Taiwan University Hospital were enrolled (33 men and 35 women; age ranged from 41 years to 91 years; mean age, 65.5 years and 65.8 years, respectively). Gefitinib was given orally as a single dose (250
mg daily). Gefitinib administration was encouraged to be continued unless the skin toxicity was unbearable and was resumed as soon as possible after the severe skin toxicity subsided. We followed up the enrolled patients for more than 30 months since the administration of gefitinib.
Clinical analysis
Cutaneous reactions after the gefitinib treatment were recorded by the oncologists, internists, and consulted dermatologists. Scrutiny reviews of the medical records, including admission note, progress notes, and nursing notes, were carried out.
Statistical analysis
Kaplan–Meier method and log-rank test were used to study the relationship between median survival time and skin toxicities. In addition to the descriptive analyses, regression analysis with multiple Cox’s proportional hazards model was conducted to evaluate the effects of age, sex, stage of disease, chemotherapy, skin toxicities, and their interactions on the patient’s survival.
15,
16 The occurrence of the skin toxicity predicting patient’s survival was further analyzed by multiple logistic regression model to discover the associated risk factors.
17 Exclusion criteria were applied in multivariate analysis to avoid confounding factors: (1) patients who expired before the median onset time of the investigated toxicity and (2) patients with the investigated reaction but the survival data as extreme outliers defined as points beyond the outer fences of boxplots. Basic model-fitting techniques for (1) variable selection (such as the stepwise method with the significance levels for entry and stay set to 0.15); (2) goodness-of-fit assessment; and (3) regression diagnostics (including residual analysis, influence analysis, and check of multicollinearity), were used in our regression analyses to assure the quality of the analysis results.
16,
17 A two-tailed
pvalue of 0.05 or less was considered statistically significant. All the statistical analyses were performed with the SPSS (Version 13.0) and SAS (Version 9.1) software (SPSS Inc., Chicago, IL, USA).
Results
Skin toxicities
In these 68 patients, 46 had skin toxicities (67.6%). The major skin toxicities were acneiform eruption (28 patients, 41.2%); xerosis (26 patients, 38.2%), generalized itching (18 patients, 26.5%), and paronychia (11 patients, 16.2%). Some other skin presentations were oral ulcers, alopecia, and petechiae (
Table 1).
Table 1. Common skin toxicities in the 68 patients receiving gefitinib therapy.
| Skin toxicities |
Median onset time (d) |
Men (%) (n=33) |
Women (%) (n=35) |
Total (%) (n=68) |
| Acneiform eruption |
14 |
14 (42.4) |
14 (40.0) |
28 (41.2) |
| Dry skin/xerosis |
50 |
15 (45.4) |
11 (31.4) |
26 (38.2) |
| Generalized pruritus |
30 |
7 (21.2) |
11 (31.4) |
18 (26.5) |
| Paronychia |
60 |
3 (9.1) |
8 (22.8) |
11 (16.2) |
Acneiform eruption usually developed on the face, anterior chest, and back, especially on the seborrheic region. Tiny pustules and/or erythematous papules (
Figures 1A and 1B) composed the eruption with similar histopathology to folliculitis. Four patients received skin biopsy, and all of them had the aforementioned findings. The median onset time was 14 days (
Table 1). Either
Staphylococcus aureus or
Propionibacterium acnes was yielded occasionally from the pus culture performed in four patients.
Propionibacterium acnes was yielded in two cases and
S. aureus in one case, and the results were negative in the other one case. The acneiform eruption was self-limited and responded well to traditional treatment for acne, such as antibiotic lotions.
The median onset times of generalized pruritus and xerosis (
Figure 1C) were 30 days and 50 days, respectively (
Table 1). Painful paronychia around fingers and/or toes (
Figure 1D) developed about 2 months after treating with gefitinib (
Table 1). Bacterial clumps over the granulation tissues were revealed histopathologically in all the three patients who received skin biopsy for this kind of lesion. In the group with paronychia, six patients (women/men
=
4/2) suffered from acneiform eruption, but another five (women/men
=
4/1) were spared. Most of the patients had only one skin adverse reaction at the investigation time. At least one of these four main skin side effects occurred in 23 of 33 men (69.7%) and 23 of 35 women (65.7%).
Skin toxicities and survival
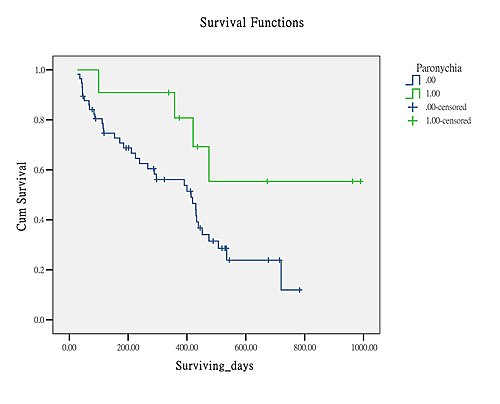
The median survival time and 1-year survival rate for patients with different types of skin toxicities are listed in
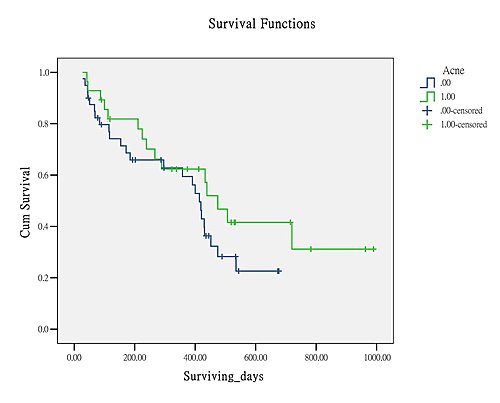
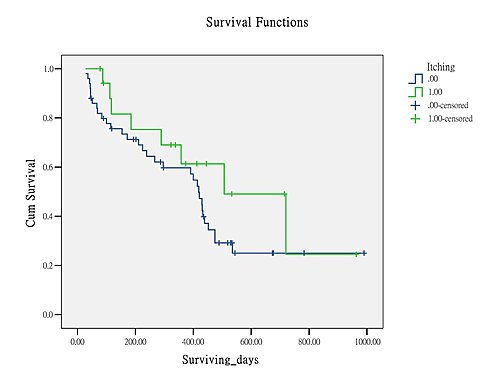
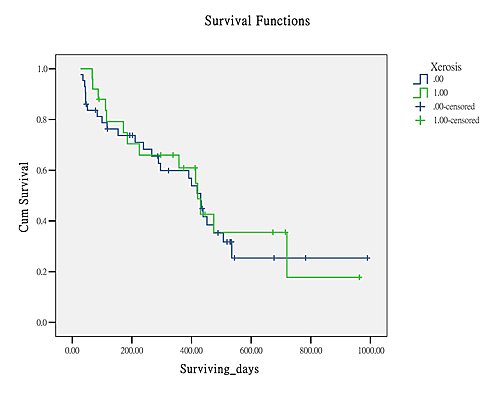
Table 2. The Kaplan–Meier estimates of the survival curves for the patients with and without each of the cutaneous toxicities are shown in
Figure 2.
18 The two-sample log-rank test was conducted to compare the survival curves between the patients with and without each skin reaction over the whole follow-up period (
Table 2).
16 This univariate analysis indicated paronychia as the most important therapeutic predictive indicator (
p=
0.0427). Statistically significant association between patient’s survival and the other cutaneous reactions were not found (
Table 2).
Table 2. Median survival days and 1-year survival rate for each of the four main toxicities.
| Skin toxicities |
Median survival d and 1-yr survival rates (%) |
| With |
Without |
p* |
| Acneiform eruption |
475, 62.4 |
414, 59.5 |
0.2022 |
| Xerosis |
421, 60.9 |
431, 56.8 |
0.7548 |
| Itching |
507, 61.4 |
414, 57.2 |
0.2509 |
| Paronychia |
Not reached, 80.8 |
408, 56.1 |
0.0427 |
∗A two-sample log-rank test was conducted to compare the survival curves over the whole follow-up period.
|

-
Figure 2
Kaplan–Meier estimates of the survival curves for patients with and without (A) paronychia, (B) acneiform eruption, (C) itching, and (D) xerosis (with: 1, without: 0). Cum survival
=
Cumulative survival rate; Surviving_d
=
Surviving days.
We considered paronychia as an intermediate variable and assumed that the stratified multiple Cox’s proportional hazards model for modeling the hazard rate of time to death (
Table 3) and the multiple logistic regression model for modeling the probability of having paronychia (
Table 4) were the equations of a two-equation fully recursive generalized simultaneous equation model (or generalized path model). Taking the occurrence of any skin toxicity as a potential “proxy” of patient’s response to the administered drug, we conducted regression analysis with multiple Cox’s proportional hazards model to evaluate the predictive effects of age, sex, staging of disease, chemotherapy, acneiform eruption, xerosis, pruritus, paronychia, and their interactions on the patient’s survival.
Table 3. Multiple Cox’s proportional hazards model stratified by stage of disease for modeling the hazard rate of time to death (n=59).*
| Risk factor |
Regression coefficient |
Standard error |
χ2 |
p |
Hazard ratio |
| Age×male |
0.0132 |
0.0068 |
3.7369 |
0.0532 |
1.013 |
| Age×paronychia |
−0.0283 |
0.0101 |
7.8727 |
0.0050 |
0.972 |
| Male×xerosis |
1.4487 |
0.5530 |
6.8641 |
0.0088 |
4.258 |
∗Grønnesby and Borgan goodness-of-fit test χ 2= 11.9445 (with 9 degrees of freedom); p= 0.2165 > 0.05.
|
Table 4. Multiple logistic regression model for modeling the probability of having paronychia (n=59).*
| Risk factor |
Regression coefficient |
Standard error |
Wald test statistic |
Odds ratio |
95% Confidence interval |
p |
| Intercept |
−2.4582 |
0.7429 |
10.9486 |
— |
— |
0.0009 |
| Male |
−1.3305 |
0.8320 |
2.5573 |
0.264 |
0.052–1.350 |
0.1098 |
| Xerosis |
2.3729 |
0.8972 |
6.9939 |
10.728 |
1.848–62.268 |
0.0082 |
∗Percentage of concordant pairs = 68.4%; percentage of discordant pairs = 10.6%; and percentage of tied pairs = 21.0%; Hosmer and Lemeshow goodness-of-fit test χ 2= 0.3733 (with 2 degrees of freedom); p= 0.8297 > 0.05.
|
To focus our multivariate analysis on the interaction of paronychia and other parameters, eight patients who expired in 60 days that was the median onset time of paronychia were excluded from this analysis to avoid underlying confounding factors. As a result, no patients with paronychia were excluded. In the remaining 60 patients, 10 patients with paronychia survived for more than 300 days, but one patient with paronychia expired on Day 100. These 10 patients were further used for the regression analysis.
With the help of the available model-fitting techniques, the fitted final multiple Cox’s proportional hazards model stratified by stage of disease (Stages 3 and 4) for predicting the patient’s survival is shown in
Table 3 (
n=
59).
16 We found that conditioning on the stage of disease (Stage 4 is worse than Stage 3), older male patients or men with xerosis have higher hazard rates of dying, but older patients with paronychia have lower hazard rates of death. Specifically, when the other variables in the fitted regression model are held fixed, the predicted hazard rate of a 60-year-old patient with paronychia would be 0.18 times less than that of a patient of the same age without paronychia according to the following calculation: exp(−0.02834
×
60)
=
0.18261.
Finally, the occurrence of paronychia was further analyzed by a multiple logistic regression model to discover the associated risk factors. With the help of the available model-fitting techniques again, the fitted final multiple logistic regression model for predicting the probability of having paronychia is shown in
Table 4 (
n=
59).
17 We found that men have a lower chance of having paronychia, but patients with xerosis have a higher chance of having paronychia, which would lead to a lower hazard rate of dying according to the aforementioned survival analysis (
Table 3). Specifically, when the other variable in the fitted regression model is held fixed, the odds of having paronychia in a patient with xerosis would be almost 11 times greater than that of a patient without xerosis because of the calculation exp(2.3729)
=
10.728. Note that the odds ratio here is the ratio of the probability of having paronychia versus 1 minus the probability of having paronychia, and thus, the greater the odds ratio, the greater is the probability of having paronychia.
Discussion
The EGFR signaling pathway is important for cell physiology and metastasis of malignancy.
1,
2,
3,
19 In human skin, EGFR is expressed on basal keratinocytes and outer root sheath of hair follicles.
20 Inhibiting EGFR-TK in vitro can induce terminal differentiation to arrest the growth of keratinocytes.
21 Cutaneous toxicities after gefitinib therapy may correlate with the significance of EGFR in human skin.
Four major skin toxicities, including acneiform eruption, xerosis, pruritus, and paronychia, are analyzed in this article. Acneiform eruption was the commonest one, followed by xerosis. Some previous studies also revealed that acneiform eruption was the most popular skin reaction,
1,
6,
22,
23 and the frequency of development might be dose dependent.
1,
22,
23 However, the cutaneous reactions were indicated as “skin rashes” in most studies without characterizing their features.
Histopathological findings in the gefitinib-related acneiform eruption showed similarity to folliculitis.
24 Activating the EGFR signaling system can stimulate the transition of hair cycle from anagen phase to catagen phase.
19,
25 The activation of EGFR can decrease the rate of growth and differentiation of multiple cell types within hair follicles.
6,
19,
20,
24,
25,
26 Gefitinib-induced follicular eruptions might reflect a disturbance of the equilibrium between follicular proliferation and differentiation.
24Excessive follicular hyperkeratosis, follicular plugging, ostial obstruction, altered follicular cycle, and subsequent inflammation may cause the acneiform eruption.
6Acneiform eruptions in our survival study did not show a significant association (
p=
0.2022) in the univariate analysis (
Table 2). However, for patients with NSCLC receiving gefitinib, who developed skin rash in any grade, a better median survival has been reported than for those without rash.
10,
12 This discrepancy may be because of the limited sample size in our retrospective study.
The second common skin adverse reaction of gefitinib in our study was xerosis. The gefitinib-induced xerosis also reflects a disturbance of the equilibrium between the epidermal proliferation and differentiation.
6,
24 Xerosis did not show a significant association with the survival (
p=
0.751) in the univariate analysis (
Table 2), but men with xerosis had a significantly higher hazard rate (
p=
0.0088) in the multivariate analysis of survival (
Table 3). As shown in
Table 4, xerosis was positively associated with paronychia (
p=